
Young Adult Hip Arthritis
Hip arthritis can affect younger patients and symptoms can be severe enough to require a total hip replacement. Some people develop hips that have shallow sockets or have abnormally shaped femoral heads or even have hip joints that have dislocated. A hip replacement is far more complicated to perform in these situations and surgical expertise is required in reconstructing these joints.
It is therefore important that your surgeon has a range of options available to him to reconstruct your hip in these situations. This may include advanced surgical approaches, custom made implants, use of bone graft or trabecular metal implants to reconstitute lost bone. I am experienced in reconstructing these joints using a variety of prostheses and techniques to create a pain-free and fully functional hip joint.

During a total hip replacement, the arthritic, damaged “ball and socket” joint is removed and replaced with an artificial joint (prosthesis). The majority of patients experience a rapid reduction in pain from the hip joint after surgery and find that they are able to move more easily and have an improved quality of life.

Through an incision over the side of the hip, the joint can be replaced with an artificial socket and a metal stem with an artificial ball mounted on the end of the stem. This is performed via a posterior approach (see FAQs) as it provides the best longevity and function for the replaced hip. I use modern implants which allow the bone to incorporate onto the implant (uncemented) and I use both ceramic, metal and polyethelene bearing surfaces tailored to the individual patient.

You will be admitted on the day of surgery having not eaten for the preceding 6 hours prior to the operation (nil by mouth). The anaesthetist will talk to you regarding the type of anaesthetic (spinal or general anaesthetic); it is preferable to have a spinal anaesthetic as there are fewer side effects, improved pain control and a speedier rehabilitation whilst in hospital. See FAQ section spinal or general anaesthetic.
After surgery patients generally remain inpatients for 1-3 days. Patients mobilise full weight bearing on the same day of their surgery and generally go home using a stick or crutch for 1-2 weeks. In the vast majority of cases, within a week after a hip replacement, patients will experience a significant improvement in their hip function.
Risk of surgery
Common
- Bleeding – Bruising following the surgery is common very occasionally a blood transfusion or iron tablets may be required. Rarely, the bleeding may form a collection within the hip joint which may require a further operation to remove it.
- Blood Clots – Deep vein thrombosis (DVT) is a blood clot in a vein. The risk of developing a DVT is greater after surgery (especially lower limb surgery). A DVT can pass in the blood stream and become lodged in the lungs causing a pulmonary embolus (see below). To limit the risk of DVTs forming you will be given stockings to wear on your legs whilst an inpatient and a daily tablet or injection to thin the blood. Moving early after surgery is one of the best ways to prevent blood clots from forming.
- Pain – The hip will be sore after the operation. Pain will improve with time and generally is much improved by the 2 week post operative mark. Rarely, pain can be a chronic problem.
- Implant wear and loosening – With modern operating techniques and new implants, hip replacements last in excess of 20 years. In some cases they can fail and this is usually as a result of the plastic liner wearing out.
Less Common
- Infection – You will receive antibiotics just before the operation starts and the procedure is performed in a sterile theatre. The wound site may become red, hot and painful. There may be a discharge of pus or fluid. This is usually treated with antibiotics and an operation to washout the joint may be necessary. In rare cases, the implant may be removed and replaced at a later date (revision surgery). The infection can sometimes lead to sepsis (blood infection) and strong antibiotics are required.
- Dislocation – The new hip is less stable than your original hip. A dislocation may occur while the tissues are healing following surgery if the hip moves beyond its normal range. The highest risk is during the first 6 weeks before scar tissue forms. If the hip does dislocate the joint will need to be put back into place without the need for surgery. If the hip keeps dislocating a revision surgery may be necessary.
- Leg Length – The operated leg may appear shorter or longer than the other. The most important requirement at the end of the operation is to produce a stable joint. Occasionally, this may involve making the leg a fraction longer following surgery. This rarely requires further treatment and often the leg may have been slightly shorter as a result of the arthritis.
Rare
- Pulmonary Embolism – This happens when a blood clot (DVT) breaks off and lodges within the lungs. It can affect breathing and is a serious condition that can be fatal.
- Poor scars – The wound may become red, thickened and painful (keloid scar). This is more common in Afro-Caribbeans.
- Nerve Injuries – The sciatic nerve is the main nerve at risk and is identified and protected throughout the operation. It can occasionally be damaged which can give rise to weakness of the foot and need for a splint while it recovers.
- Fracture – Bone may be broken when the new implant is inserted. This may require fixing during the operation and could result in protective weight bearing for a few weeks after surgery.
- Blood vessel injury – Blood vessels around the hip may be damaged, this can require further surgery by the vascular surgeons
Robotic Surgery is the future in joint replacement surgery
The use of robotic technology has several benefits.
- Improved accuracy and precision – There is always a small chance of human error in any operative procedure, robotic assistance adds an extra level of accuracy and precision to the surgery1-4.
- Increased consistency – In conjunction with being more precise, robotic technology is more consistent than conventional methods5.
- Reduced complications – The technology enables precision implantation of the socket component to the nearest degree and enables recreating a patient’s correct leg length and offset to the nearest millimetre. This degree of accuracy improves the postoperative results and reduces the risk of dislocation and leg length discrepancy.
- Greater chance of restoring movement and mobility – As a result of a smaller incision, less soft tissue releases and greater accuracy of implantation many patients experience reduced recovery periods as well as an increased chance of restoring freedom of movement and complete mobility.
These benefits result in improved outcome metrics
- Better patient outcomes – It has been shown that patients who receive robotic surgery report better functional outcomes and experience fewer readmissions to hospital. They also require less rehabilitation than patients who undergo conventional hip replacement.
- Higher patient satisfaction – patients can return to their daily activities and work sooner after robotic hip surgery and this translates into improved patient satisfaction ratings.
- Lower long-term costs – Patients who receive robotic hip surgery tend to have fewer complications meaning less return visits to hospital. The CORI™ robotic system is an image free preoperative mapping system eliminating the cost and implications of a CT or MRI scan6. Patients also recover quicker and are able to get back to work sooner.
Is Robotic hip replacement surgery better?
Yes. Robotic surgery has been shown to deliver better results compared to conventional hip replacement. Improved accuracy, consistency and more reliable recreation of leg length, offset and cup positioning following a CORI™ robotic hip replacement result in better patient outcomes.
Metal on metal hip resurfacing is an operation that lost its popularity in the 2010s due to significant complications associated with metal debris generated from the bearing surface1. The metal particles that were released caused considerable damage to the soft tissues and resulted in early failures of the hip resurfacing implant which required revision (redo) operations. Due to the extensive damage to the bone and soft tissues around the hip, the functional outcome following revision for a failed metal on metal hip resurfacing was often poor.
As a result, there has been a significant decline in implanted hip resurfacings from its zenith in 2012 where 10% of hip replacements were resurfacings to current day where 0.1% of hip replacements are hip resurfacings2. This decline in its use is not just to do with the metal on metal complications but also a result of conventional hip replacements having improved both in terms of biomaterials and surgical techniques.
However, hip resurfacings have inherent advantages in certain patients over conventional hip replacements – in particular younger and more active patients as Andy Murray is testament to3.
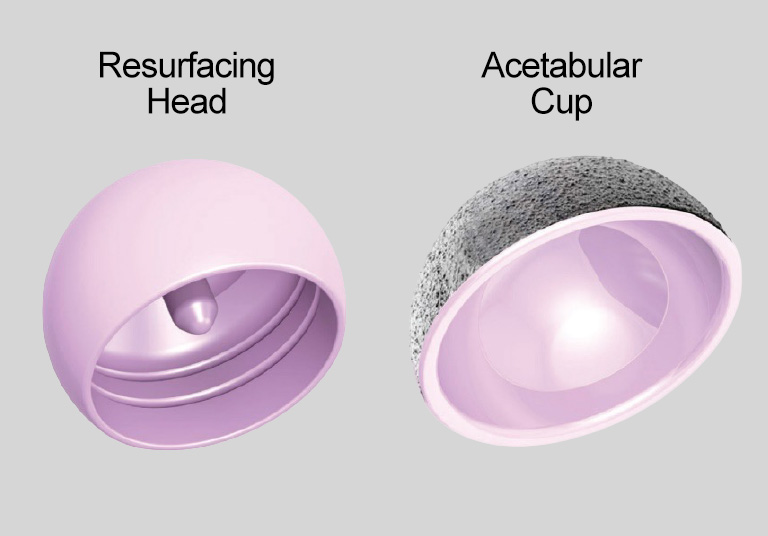
The next generation of hip resurfacings that I use avoids the use of metal bearing surfaces as they are ceramic bearing therefore patients are not exposed to the risks associated with metal wear but still experience the benefits of a hip resurfacing.
The Benefits of Hip Resurfacing
- Reduced risk of dislocation - As the femoral head is resurfaced (not replaced) it is the same diameter as the natural femoral head and as such much larger than a conventional hip replacement femoral head. This makes the joint more stable and allows for more vigorous sporting activities that involve repetitive impact loading.
- Restoration of normal biomechanics – With a resurfacing procedure the biomechanics of the hip joint are not altered and therefore patients tend to have better restoration of biomechanical function.
- Revisions are easier – Over time hip resurfacings like hip replacements can wear out particularly in young active patients who have used their replacement to the fullest degree. Revising a hip resurfacing when it has worn out tends to be an easier revision than revising a total hip replacement.
The ReCerf ceramic resurfacing implant received its CE mark for European use in Summer 2025 and the two year clinical results have been published.

Bringing back hip resurfacing without the associated risks that metal on metal bearing surfaces expose patients to is exciting. If you would like to discuss whether ceramic hip resurfacing could be an appropriate operation for you, please contact Ben Spiegelberg 0208 736 4614.
- Pseudotumours associated with metal-on-metal hip resurfacings. H Pandit1, S Glyn-Jones, P McLardy-Smith, R Gundle, D Whitwell, C L M Gibbons, S Ostlere, N Athanasou, H S Gill, D W Murray. JBJS[Br]. 2008 Jul;90(7):847-51. PMID: 18591590
- National Joint Registry (NJR) - 22nd Annual Report 2025 - The National Joint Registry
- Andy Murray: What did his surgery entail, and what is his long-term outlook? - BBC Sport
- Two-Year Results of Ceramic-on-Ceramic Hip Resurfacing in an International Multicenter Cohort. D Lin, J Xu, P Weinrauch, D Young, K DeSmet, A Manktelow, P Beaulé, W Walter. The Journal of Arthroplasty. Vol 39, Issue 11, Nov 2024, 2800-2806